It's the first non opioid painkiller applicable for situations like post operative use.
I'd have loved this after my hernia op, the last thing you need with that is opioid induced constipation.
Yes, but:
> Responsible for 56,000 emergency department visits and 2600 hospitalizations, acetaminophen poisoning causes 500 deaths annually in the United States. Notably, around 50% of these poisonings are unintentional, often resulting from patients misinterpreting dosing instructions or unknowingly consuming multiple acetaminophen-containing products.
Source: https://www.ncbi.nlm.nih.gov/books/NBK441917/#:~:text=Acetam...
Thing is, as we are a popular destination with British tourists or even pensioners that live in the Mediterranean, we've found in the last years that British population is genetically more likely to have a very dangerous side effect, agranulocytosis, that could result in death.
Can't find the exact source (I'm on my phone), but seems like at least half of the metamizol related agranulocytosis cases in Spain have been of British origin, and several deaths have been reported. There's a ongoing legal process where at least 40 deaths are being investigated [1] and doctor have stopped providing metamizol to persons of British origin, and do it carefully for other persons.
So what was perfectly safe around here, was found quite dangerous for certain subset of the British population (no jokes about balconies, please).
Edit for some sources:
From 1998 to 2003, out of the 13 agranulocytosis cases from a hospital in Marbella, 8 were foreigner, and of those 5 were from the UK [2]. According to the ADAF association, out of the 45 deaths attributed to metamizol in Spain since 1996, only 8 of them were Spanish (they don't tell their sources in that article) [3]
--
0: https://fefe.com/wp-content/uploads/2023/05/Obs.-marzo23ok.pdf
1: https://guardian.pressreader.com/article/281857238286709
2: https://www.sciencedirect.com/science/article/abs/pii/S0014256509713104
3: https://www.elespanol.com/ciencia/salud/20231128/denuncian-sanidad-muerte-decenas-britanicos-espana-tomaron-nolotil/812919101_0.htmlDoes the UK have rules that prevent mixing acetaminophen with other drugs? Its getting so its sometimes hard to find over the counter cold/flu medicines without acetaminophen
Non-pharmacy retailers are only allowed to sell in packs of 16, and they'll usually only allow two packs of any paracetamol-containing medication to be sold at a time (eg. one cold/flu and one cough remedy).
If the name of the product doesn't already contain the word "paracetamol", then all of the packaging must prominently display "contains paracetamol" - so even small retailers that don't have computerised checkouts are expected to follow the same rules.
Deaths from paracetamol overdose fell by 43% (with a similar decrease in the rate of accidental poisonings) in the first 11 years after these changes were implemented: https://www.bmj.com/content/346/bmj.f403
Trying to find medicine for her when she's sick is surprisingly time consuming as it is in so many things even vaguely related to treating cold / cough / flu symptoms.
Score one for the nanny state.
Teach a man why not to over-fish fish vs giving him a smaller amount of fish... or something.
I'm willing to bet that handing out cyanide pills OTC would effectively eliminate intentional acetaminophen poisonings in the UK. Surprised the boffins at the NHS didn't think of it first if they really want to eliminate intentional overdoses! /s
The vast majority of adults should be able to live in a world where they're not treated like 10-year-old children for seeking a bit of modest pain relief for very common ailments.
Fifty thousand hospital visits per year
> isn’t reasonable
Fortunately this is not a popular opinion
There were over 50,000 hospital emergency room visits, yes. However, bear in mind that many thousands of people visit emergency rooms for all kinds of unfounded reasons every year anyhow. Of those 50,000+ paracetamol-related visits (speaking of the United States here), less than 5% resulted in any need for hospitalization and only 450 or so deaths were registered in 2023, as a recent example year. These numbers out of an estimated 60 million individual uses PER WEEK by Americans according to the NIH.
For some perspective, accidents caused by "Fall involving ice-skates, skis, roller-skates or skateboards" in the U.S cause an average of 1000+ deaths per year.
Paracetamol can, just like many drugs, be dangerous, but if your criteria for paranoid restriction of something so commonly necessary and used without problems in the extreme absolute vast majority of cases are the numbers above, you'd better start banning one enormous shit list of completely innocuous activities and things that normal adults have access to before you reach something like paracetamol.
There seems to be a sort of mental illness prevalent in the kind of logic that equates any evidence of self-harm with a given product or thing with a rabid need to treat people like children in their access to it.
The entire adult population should not have to be treated like drooling morons in their very most basic personal medical choices because a completely minuscule percentage of the population lacks the mental capacity to read a basic safety label for a common medicine, or control their childrens' access to something that's easy to keep away from them.
> In adults, single doses above 10 grams or 200 mg/kg of bodyweight, whichever is lower, have a reasonable likelihood of causing toxicity.
10g is 20 pills of the highest strength you'll find in a regular store. Excedrin brand "Extra Strength" is half of that, you'd have to be eating 40+ pills in 24 hours, or 20+ pills per day on multiple consecutive days. Most acetaminophen pills have 100-200 mg of the active ingredient.
You're missing the context:
> Intentional overdosing (self-poisoning, with suicidal intent) is frequently implicated in paracetamol toxicity.[25] In a 2006 review, paracetamol was the most frequently ingested compound in intentional overdosing.[26]
So, it's not that acetaminophen will kill that easily. It's just that of the easily available ways to kill yourself, it's distinctly the one that destroys the liver quick.
The reason for the rule though was to combat its use in suicide attempts. They also have to be sold in blister packs here for the same reason, not the big bottles of Tylenol/Advil etc. that you get there (and we used to here) - relatively difficult to take several, requires more preparation than just chugging a bottle.
> During a median follow-up of 12.3 years, 6407 (3.0%) participants developed new-onset all-cause dementia. Participants who regularly used paracetamol had a significantly higher risk of new-onset all-cause dementia (adjusted HR, 1.18; 95%CI: 1.10-1.26), compared with non-users. However, there was no significant association between regular use of ibuprofen and new-onset all-cause dementia (users vs. non-users; adjusted HR, 1.06; 95%CI: 0.97-1.16).
I don't follow the research closely enough to know if this is reliable evidence, but there are other studies showing the same thing.
Paracetamol also well known as mood-altering, apparently inhibiting empathy [2], which may be part of why it has an analgesic effect. That isn't as scary on a personal level, but imagine a society full of millions of people on paracetamol whose ability to feel empathy has been blunted.
Worse than that: it is effectively per day per shop. In a very short space of time I can buy two packs in Boots, two in Tesco, two in Sainsbury, ooh look another small Tesco I'll get two there as well, two from Savers, two from SuperDrug, …
It's essentially just raising a barrier for (under normal circumstances) undesirable behavior.
It doesn't do what it is sold as doing¹ while causing a bit of faf.
The restriction is one of those put in place because someone somewhere want to be seen to be doing something.
> for (under normal circumstances) undesirable behavior.
Outside of a supply problem situation, which we don't have for that sort of thing and different at the time the change came in, why is it so undesirable?
--------
[1] Reducing accidental overdose rates², reducing people using out-dated-so-possibly-ineffective medicines, etc.
[2] Accidental overdose rates have fallen, but they have in many places without those restrictions, so I suspect that is a coincidence and probably more due to greater awareness³ of there being paracetamol or aspirin in other products and therefore the need to be careful what you take in combination.
[3] Due to better labelling?
I think it's important to recognize that overdoses can be intentional or unintentional, and it isn't clear which ones will be affected by the policy of limiting purchase quantity per transaction.
The US went with the educational route - any product containing acetaminophen has “CONTAIN ACETAMINOPHEN - DO NOT COMBINE WITH OTHER PRODUCTS CONTAINING ACETAMINOPHEN”
Overdoses went down despite the fact I can buy $1,000 tablets for $5 at Costco.
The fact that another country had success with a different technique too doesn't mean it wasn't successful.
"The downward step change was not apparent when the intervention point was moved back to the beginning of 1998."
"Despite the apparent benefits of the 1998 legislation, there continues to be a considerable number of deaths each year due to paracetamol poisoning"
"One limitation of this study was that we only used data for deaths for poisoning with paracetamol (with or without alcohol), in pure or compound form. We did not use data for deaths where paracetamol was consumed with other drugs."
They had to take the available data and massage it like a Thai masseuse to find what they were looking for.
Not to mention they estimate a decrease of 7 deaths per year, where the post-change level is 121 deaths per year. That's a 5% change, so it's not surprising they had to look at the data a number of ways to even find a change.
This 2017 study I found in 30s of searching is seemingly underpowered at n=30 or so, but the (preliminary) implication is awful enough that I won't give my boys ibuprofen at all. Out of abundance of caution.
They can have naproxen or acetaminophen instead -- we keep those out of reach and teach our children not to touch them without adults.
Perhaps there is some more recent research?
Again and again, this hepatologist makes his message clear: "Acetaminophen (Paracetamol) is the safest anti-fever and anti-pain medicine even among patients with liver disease. It is the first choice for fever and pain management even in advanced cirrhosis."
Look for some of his other posts on the topic for studies and citations.
I take acetaminophen, but only occasionally.
And the people that have serious toxicity at 5 g are likely already sensitive due to alcohol intake, malnutrition, etc.
For a healthy, well fed human who isn’t consuming alcohol the dose that causes serious issues is closer to 20x
Me: yep argued with some strangers on HN about how daft/wise UK's paracetamol laws are, highly fulfilling!
:-)
Its introduction pretty effectively reduced the incidence of suicide attempts by overdose resulting in death or hospitalisation.
https://pubmed.ncbi.nlm.nih.gov/23393081/
(The tl;dr conclusion: it worked, consider going further.)
Acetaminophen and paracetamol are two names for the same generic chemical composition drug, which is why it is especially confusing. You can ask for aspirin or ibuprofen in any English speaking country, and they'll know what it is, but the world is divided on which of the two generic names to use: some acetaminophen, some paracetamol.
FWIW, acetaminophen was coined a year earlier than paracetamol, much like soccer was the accepted term far prior to football, but the Brits and a fair few other countries choose the later versions of the words.
From Association Football we get soccer. So Football was first then soccer.
e.g. The Football Association was formed in 1863 and the first international match in 1872 was billed as International Foot-ball Match and then in small writing (Association Rules) before the term soccer was used.
Perhaps the first approved by FDA, I don't know. In many countries, metamizole is the first-line drug for postoperative pain.
(It should be noted that metamizole may very rarely cause agranulocytosis. It is suspected that the risk varies depending on the genetic makeup of the population, which would explain why it is banned in some countries but available OTC in others.)
Tangential: China technically banned metamizole due to the agranulocytosis scare, but somehow small clinics always have fresh stocks of this stuff. And their stocks don't look like my metamizole for horses! It's pressed out of the usual magnesium stearate instead of whatever rock-hard thing they use for animal drugs in China.
I had kidney stones last year, by far the most painful thing I have experienced, and got opioid based painkillers which made me constipated. To try and fix that I was eating some stoned prunes and it turns out one of them wasn't stoned and I damaged a tooth (it was weak anyway and needed replacement with an implant).
It's a NSAIDs but it's not to hard on the stomach but it's somewhat hard on the kidneys. However Ketorolac is a dangerous drug if you don't follow the posology (don't take 2 pills at the same time, the therapeutic index is that narrow) or if your a poor metaboliser, it leads to kindey failure, stomach bleeding and other life threatening side effects. I would be surprised if that new pain killer was superior to this.
I am sure it's less dangerous but more effective I really doubt it.
https://medicalxpress.com/news/2025-06-acetaminophen-discove...
https://pubmed.ncbi.nlm.nih.gov/27217114/
https://pubmed.ncbi.nlm.nih.gov/32888031/
My primary care doc doesn't want me taking either NSAIDS or acetaminophen so when I get asked at the urgent care what I take for pain I say "Nothing".
Well, not nothing, my stomach clearly doesn’t like it and I feel it.
Human pain and painkillers response seems extremely variable across different subjects.
After what felt like an eternity, I myself noticed a wetness on my shoulder onto which a broken hose adaptor had leaked. After that was replaced, there were no further issues. Thankfully, the stitches had held, and I didn't get a hernia.
Also, I did have to carry a pee-bag while the epidural was in, because the epidural made me lose control of my bladder. And the epidural itself left a scar.
Meanwhile my understanding of Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) was that they were exactly that by definition - Anti-Inflammatories with pain being reduced by reducing the immediate cause of it, inflammation, not by interfering with the actual mechanisms of pain.
I guess one could consider general anaesthesia (laughing gas, ether, and more modern successors) to be "painkillers" too but they're obviously not quite the same category of thing.
Anyway, I enjoyed the article - it would be interesting to hear the author give their own reasons for not accounting for NSAIDs.
NSAID is effectively a shorthand for COX inhibitor; the term NSAID was coined at a time when the mechanism wasn't fully understood, and all other anti-inflammatories were steroids.
Paracetamol does target COX-2, but does so in a way that doesn't really have any effect on inflammation. Its main mechanism of action is as an AM404 inhibitor.
If you ask me whether I choose pain or constipation, well, I am pretty sure you know the answer.
This constipation goes away once you stop, and everything depends on the dose and the frequency and duration of taking it.
In the US it seems like they prescribe opioids like candy. I've never heard of opioids post hernia surgery in Europe.
Plus some sachets of laxative for any constipation.
There has been a huge opioid epidemic there as well.
Plus don't forget: even the "pain relief" provided by sticking a knife through your skin to the bone is addictive. So the side effect of addiction isn't going to go away.
> the side effect of addiction isn't going to go away
While I agree with your conclusion itself, I disagree that the premise implies the conclusion. The main difference between suzetrigine and opioids, as explained in the article:
Crucially, opioids don’t just kill pain: they also incite pleasure.
When the mu opioid receptors present in the reward center of the
brain are activated, this reduces the secretion of a neurotransmitter
called GABA, which works to inhibit dopamine-producing neurons. As GABA
release declines, dopamine spikes, lighting up the reward center and
inducing pleasure.
Since suzetrigine doesn't affect mu receptors in the brain, this mechanism doesn't apply.
But I'm almost sure it will have some other unintended side effects. Morphine had them, heroin had them, methadon had them... And each time the inventors were sure they didn't.
LOL, this thread just keeps on delivering.
Injuries generally cause brain to release endorphins, which in turn releases dopamine, causing addiction. For example, cutting is a common type of self-mutilation depressed people do. High-intensity exercise arguably also does the same thing - as your body is "microinjured" by strain, your brain releases endorphins to help with the pain, causing effects like "the runner's high".
And the Internet is the place where you get exposed to them at random.
Like for Aron Ralston, who was trapped under a rock and had to cut off his own leg to escape: would it have reduced his pain if he had stabbed himself in the shoulder to the bone?
Would this best be done with, say possibly, acupuncture needles or an ice pick, so as to minimize the damage and to maximize the relief?
Gunsmoke TV episode:
Doc: Well, Billy, we'll have to amputate your lower left leg - it's shot plumb thru with gangrene.
Billy: Will it hurt, Doc?
Doc: Hell yeah, it'll hurt! But thanks to Hacker News we have a new pain treatment: every time you yell. Chester here will stab your right leg to the bone with this h'yar ice pick. And Mary will hold a leather strap in your mouth so your teeth don't crack off! Don't forget to breathe.
Billy: I'm obliged and grateful to be part of your research program, Doc, but can't you instead just wait 10 minutes while I drink this here quart of whiskey and pass out? Then you can do as you wish.
Doc: Hell, no, time's a'wasting! Hold him down, fellas! Doctorin' progresses only a step at a time!
> The first non-opoid [sic] painkiller
might be:
> The first non-opioid nociceptive pain-killer
Nociceptive pain being that by actual damage to tissue, as opposed to neuropathic pain like a headache or inflammation that you might take a (non-opioid!) NSAID for.
Inflammation would be an instance of nociceptive pain, and an NSAID would alleviate it by reducing the inflammation; and most tissue damage will result in inflammation.
Neuropathic pain, on the other hand, would be due to damage of the nerves themselves, and NSAIDs are completely useless here (ask anyone with sciatica or other nerve entrapment)
Perhaps non-inflammatory (or generically) nociceptive pain killing is the point. (Which is getting a bit specific for such a broad title isn't it. Does 'painkiller' ordinarily have such a narrow meaning in your experience?)
The point isn't to accurately describe it as 'nociceptive' (which I've never heard of before either) and have that be understood, it's to qualify it such that it isn't confusing or sounding like an historical tale of how whatever the first NSAID/analgesic was came to be.
My wife, daughter and I are very pain tolerant. Out of curiosity, I've turned down freezing for fillings and I even turned down some of pain meds before abdominal surgery. I've never taken the post op opioids, including when I had my impacted wisdom teeth removed.
My other kid, on the other hand, is a whimp. She gets anxious simply if I replace her earrings.
My use case for anesthesia is very different from my kid. I struggle to appreciate why anesthesia is even necessary beyond the need to restrain the patient.
My kid could go into a full blown panic attack from pain.
Yet I don't see anesthesiologists ever asking "how good are you with pain?"
In physiotherapy, we used to think that structural issues like slipped disks caused pain, but when we started imaging healthy people, we found the same structural issues commonly in the 'healthy' population.
Both how much pain we feel and how sensitive we are to it are things that can be learned. The bullet ant initiation rites of the Sateré-Mawé people are an extreme example.
A decent book on this is 'dopamine nation'.
You'd think my comment's thesis that folks with lower tolerances should be respected and treated differently would have given the rhetorical device away.
Really not sure how to feel about this part lol, I mean I get it, but at the same time this is very ugh.
If you remove the flag (pain), harm will continue.
I worry a lot about aging, and I'm also afraid of things like tumors or cancers that I might not feel until it's too late. As an example, I can't feel cavities forming and I didn't even notice my wisdom teeth piercing through my gums when I was a teen.
Many years later we found that the actual cause was a Cerebrospinal Fluid (CSF) Leak.
After two failed surgeries to fix it, she had enough and checked herself out.
See our documentary Pain Warriors for the whole saga.
That said, the article may not be fairly representing what happened in the first place, so...
Clicking "FDA" in the bit you quoted above takes you to a different page wherein the FDA laments the lack of data around the drug (eg, the "hypothesized mechanism"). It also suggests that the companies intend to work with the FDA more on this.
Was the vote against approval a move to "completely prevent a drug from entering the market and being used", or was it a desire to better understand it before saying "okay"?
Why do you present this as an either/or?
> Clicking "FDA" in the bit you quoted above takes you to a different page
Indeed, where I found that...
> That said, the article may not be fairly representing what happened in the first place, so...
...this is exactly what happened, i.e. I was successfully misled even before reaching your false dichotomy. Yay.
>... your false dichotomy.
I appreciate you giving me the opportunity to answer your first question before coming to the conclusion that I was using a false dichotomy.
I didn't intend to present it as an "either/or", though I can see how it can be read that way. I simply read you saying that they "completely prevent[ed]" something from coming to market when, perhaps, they're not "completely" doing anything and are open to doing it provided that they know more about it. That the "incomplete justification" you lamented may also have been how the FDA felt about the data provided to them.
It could also be for other reasons, absolutely! This is just one possibility that seems very obvious to me. There's no either/or from my end.
If I didn't already conclude that you presented a false dichotomy, why would I have inquired about why you did so? It's also not set in stone; from your reply I can just change my mind afterwards. But why do it in two rounds when I can do it in one?
I understand if I came across as hostile though, I admit it was sadly reflexive, and I apologize.
> perhaps, they're not "completely" doing anything and are open to doing it provided that they know more about it.
That's not a nuance I intended to disregard. Yes, I understand they can revisit the drug's approval later, didn't mean to suggest otherwise.
Gosh I hate natural language sometimes.
Especially when it's sometimes hard to read tone, even moreso from a stranger whose communication style we're unfamiliar with. Even harder still, comments online generally don't lend themselves well to nuance and assumptions can easily be made, such as my leaning too heavily on your use of the word "completely"! Should we hug it out?
Hope you enjoy the rest of your day. :)
The more I learn about pharmacology, the more I realize this is the norm, rather than the exception.
https://www.sciencedirect.com/science/article/abs/pii/S03785...
And that's not even taking into account its cardioprotective effects.
But hey, it can be hard on the stomach in SOME people so we developed alternatives with all sorts of nasty side effects, up to and including heart attacks and strokes (rofecoxib, valdecoxib, etc.) Hell, a decade ago, the FDA issued an advisory across the board that "Non-aspirin NSAIDS increase the risk of heart attacks and strokes":
https://www.fda.gov/drugs/drug-safety-and-availability/fda-d...
Some day we will look back on the attempted replacement of aspirin with these other drugs the same way we now look back on the replacement of butter with margarine (and the replacement of saturated fats with trans fats more broadly).
The agency bears zero responsibility for the pain and suffering its caused by overcaution.
Thalidomide.
Patients (and often doctors) really don't have the skills or information to make an informed decision.
They can however have 'feelings'. This is not the same thing.
To continue my example of thalidomide, the FDA's Dr. Frances Oldham Kelsey prevented millions of American babies from being born with devastating deformities.
At the same time millions of American mothers and their GP's were clamoring for the anti-nausea drug that the British mother's were enjoying. And they too said the FDA was getting in their way.
Experts aren't "made of finer clay" : they just know a lot more than the populace about specific topics. There are other topics where I am the finer clay. See 'specialisation'.
Especially when the article itself compares it to ibuprofen:
> If paracetamol and ibuprofen are inadequate for pain relief, Journavx can now be prescribed as the next alternative treatment, instead of mild- to moderate-strength opioids.
"suitable for treating post-surgery pain" isn't something to cut, just for a better title. It just makes the clickbait stench of that first line even worse.
This is a better paracetamol. Which is awesome, and something we need. This is not a world first.
You can take them together within the stipulated limits for each, as one will reduce inflammation and the other will reduce the perception of pain.
Just have to be careful with the stomach when it comes to Ibuprofen... perhaps eat first.
More often used for neuropathy than epilepsy (though used for both, due to how gabapentoids work.)
Did I miss something?
EDIT: answered in sibling post, thanks @ggm!
[1]: Non Steroidal Anti-Inflammatory Drugs
I believe it's still somewhat legal for consumption in the U.S., though other countries have been moving to ban it to varying degrees, since it can be used recreationally, though it isn't known to produce the same intensity of euphoria as opioids, and can also be addictive, though I don't believe it to produce as severe withdrawals as opioids.
All in all I think it's a sadly understudied and underutilized medicine, which is the unsurprising result of pharmaceutical companies having less incentive to study plant medicines
I'm really of the belief that the only reason kratom exploded in popularity the way it did was because it was a legal alternative to opiates. Not necessarily because it's an upgrade (or even sidegrade. ) If morphine could still be purchased in every corner store and pharmacy over the counter kratom extracts would never have blown up the way they did.
The term 'painkiller' is reserved for strong pain relief, and wouldn't include things like ibuprofen. That made me think immediately of a non-opioid pain blocker not just a pain reliever.
Having claimed it was cultural. It have been helpful of you indicated which culture you felt this applied to.
In UK I'd say painkillers includes ibuprofen and paracetamol. I suppose with ibuprofen it's also referred to as an anti-inflammatory. Not sure how else one would refer to paracetamol other than with synonyms (analgesics) or euphemism (pain relief tablet).
I particularly disagree with the parent comment that calls this click bait. The topic's intrinsically interesting to anybody who'd be lured in by that title; it doesn't need "bait" and we all know NSAIDs exist.
The article's particularly good at citing its references inline, which I very much appreciated. Added this author to my RSS reader in fact.
Maybe there's some very specific, limited medical context where this is the case but in common parlance it's not at all the case, search for "painkiller" in an online shop like Amazon and you'll find a whole lot of Paracetamol/Tylenol, and various NSAIDs (aspirin/ibuprofen) and manufacturers of those drugs actually use that specific term.
In which dialect of English do you think this is true?
https://www.painnewsnetwork.org/stories/2024/12/23/more-lack...
As someone else already mentioned in this thread, in Europe there is already metamizole which is used for post-surgery pain. Anyone knows if suzetrigine is more effective than metamizole?
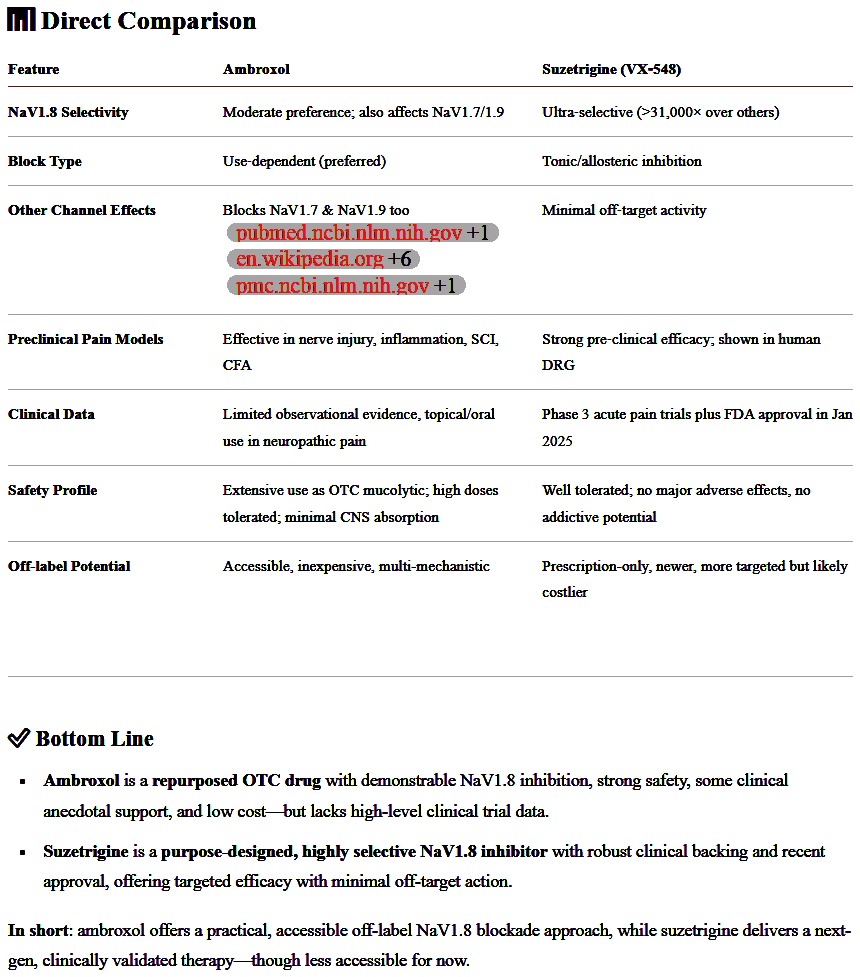
They are both Nav1.8 blockers, but in Germany you can get lots of ambroxol for cheap and OTC.
Really appreciate you mentioning it
It potentiates antibiotic effect in lung infections, including tuberculosis, treats painful hyperacusis, trigeminal neuralgia, neuropathic pain, parkinson, gaucher disease...
...and what's this? We have a surprise guest!
Ambroxol significantly reduces snoring and thus suddenly becomes a candidate for a medication half the population should take!
https://www.researchgate.net/publication/314424871_Evaluatio...
It's one of those drugs that deserves way bigger interest than it gets.
https://images2.imgbox.com/e1/b7/YaB8gjLI_o.png
but apparently the problem with ambroxol vs suzetrigine
is it is not as selective on the ion channel and not as strong (needs megadose to do similar)
I cannot remember the drugs offhand but this is the same problem with other old generics for other kinds of targets
suzetrigine won't be generic for years which is a shame
technically Low‐Dose-Naltrexone (aka LDN) is not an opioid and reduces pain
(however it does it by modulating opioid receptors so okay I guess it's opioid-related)
found more background here
https://www.newyorker.com/magazine/2025/06/02/the-radical-de...
If you want to see what a "non-addictive" painkiller is like, watch Dopesick.
A government agency with very high trust that partners with companies and helps to get things approved but only when they’re safe and has gotten more efficient since Covid is a rare and precious thing.
Which is why some bean counter or ideologue cutting this stuff will halt progress all over the place.
Having said that, ketorolac is a very potent pain inhibitor, can be prescribed for 6 days, causes no dependence issues. Pretty sure can be prescribed more. Cheap, out of patent protection. Took it when broke my hand, it was a miracle of painkiller.
This is a silly headline.
Huh? How can a compound contain another compound. I thought opium was the term for an extract which contained opiates (compounds) and not the other way round.
---
"Opium" is the dried latex (milky fluid) that comes from the seed capsules of the opium poppy (Papaver somniferum).
Opium contains ~12% morphine, ~2.5% codeine, and ~1.5% thebaine, all of which are analgesic alkaloids that act on the μ-opioid receptors. So opium itself is a cocktail of these, plus non-analgesics like noscapine (a cough suppressant) and papaverine (a vasodilator.)
Heroin is synthesized from morphine by acetylation.
Oxycodone is synthesized from thebaine in a more complex, multi-step process.
As for the terms "opiate" vs. "opioid", the terms are sometimes used interchangeably but "opiate" generally refers to naturally occurring chemical (morphine, codiene, thebaine, etc.) while "opioid" is a catch-all Heroin is often lumped in with the opiates since it is a simple synthesis; oxycodone could be called a "semi-synthetic" opioid, and fully synthetic opioids include fentanyl, methadone, and tramadol. Relative to morphine, codeine is about 1/10th the potency, heroin is 4x, fentanyl is 50-100x, and the veterinary analgesic carfentanil (given to elephants and rhinos) is 10,000x--yikes!
Wikipedia:
> At least 100 distinct phytocannabinoids have been isolated from cannabis, although only four (i.e., THCA, CBDA, CBCA and their common precursor CBGA) have been demonstrated to have a biogenetic origin.[6] It was reported in 2020 that phytocannabinoids can be found in other plants such as rhododendron, licorice and liverwort,[7] and earlier in Echinacea.
Cannibinoid receptors are separate from opioid receptors.
Seams strange if this one truly will not have "drug abuse" connected to it.
There are also lots of studies indicating that the speed of action of a drug is important for addiction. Which essentially boils down to the fact that the brain (beeing effected by operant conditioning) needs a drug response that is sufficiently noticeable to be connected to the action of taking the drug.
{kind=link}