Ongoing study: https://pubmed.ncbi.nlm.nih.gov/39780249/
Usual rant to news outlets: Cite your damn sources! (if they are public, which is the case here). This is a web page, not printed paper, web pages support links, links are not just for ads!
I know all the cynical reasons not to do it, but I feel like even the good faith objection has a pretty straightforward solution.
That's why when you click on a link you see 1/10th of the article, and then a video, and 3 other irrelevant inlays for other links.
Oh and the video auto plays with sound.
And every word in the article that is remotely a 'tag' links to other parts of the website.
- Rybelsus (type-2 diabetes; oral semaglutide 14 mg/day; much less bioavailability)
- Wegovy (obesity; injectable semaglutide 2.4 mg/wk)
- Ozempic (type-2 diabetes; injectable semaglutide 1.0 mg/wk)
For details, see: https://pubmed.ncbi.nlm.nih.gov/38921025
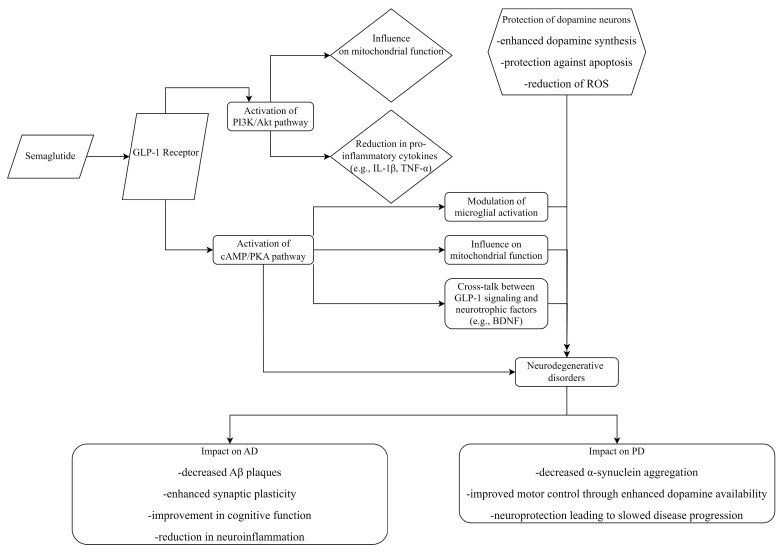
This diagram shows how Ozempic can produce these results, the various pathways from the GLP-1 receptor to reduce inflammation, protect neurons, and affect mitochondria: https://cdn.ncbi.nlm.nih.gov/pmc/blobs/87c0/11202139/72234dd...
You could think of it similar to a study that shows something like "People who don't watch network TV have fewer strokes", which could be an interesting correlation, but the causal effect might be something more like "people who are more health conscious tend to avoid sitting down for extended waking periods" which ultimately has nothing to do with TV.
But you could speculate that obesity -> cardiovascular issues -> neurological damage, and that could explain things.
Edit: I mean in the theoretical “this targets the x receptor” kind of way, not in “we tested this and found no causal link” way.
So i can see the correlation for T1D and undiagnosed T2D cases Alzheimers. Now having a parent with both T2D and Alzheimers when they were taking rebelsis there was a change in their overall mood and activity , but i saw the change was "hey your sugar is under control, and no i am not your buddy from the army" . To be clear the difference is the fog of being unclear about what's going on like you're drunk , vs the grand delusions of seeing a different person that's not there .
This should have been obvious for the researchers.
That's why they do research, to find out instead of just guessing.
This could just be false though, I can't recall where I heard this information. So do some searching before quoting me.
People who play armchair doctor only make things worse for those of us who are actually disabled.
That said, I’m not going to share details with you because your other comments in this thread indicate that you intend to argue in bad faith.
However, if anything I said seems interesting, feel free to google! The bio-psycho-social model is very interesting, it’s the first real advance in pain management since we lost opioids as an option.
These kinds of disorders — the ones you think aren’t real — are really disabling. I genuinely hope that you (or really anyone) never find yourself in this position, it’s truly miserable.
I don't notice them. Do you have numbers to back this up?
> that would be solved if they started an aerobic and strength training regimen.
Source?
I don't notice an absurd number of young, frail people or young people with canes. There are a larger number of people of all ages masking than was the case pre-pandemic (especially outside of the ethnic groups where precautionary masking was common pre-pandemic) but...I don't think that's particularly a sign of changes in health status as it is of changes in perception of external environmental conditions and associated health risks.
Another problem it seems to help with is addictive/impulsive behavior. This might lead to wrong choices in diet or activity.
I suspect that many many functions of the body are degraded or disabled by too much weight or wrong choices, and fixing those problems might let the body cure and maintain itself properly.
https://www.alzheimers.org.uk/about-dementia/managing-the-ri...
- [1] https://www.astralcodexten.com/p/why-does-ozempic-cure-all-d...
Glp-1 drugs inhibit drinking and compulsive behaviors and I'm not sure the mechanism of action is known
I'm sure this isn't the last we will hear of the potential of GLP1s in neurological diseases.
At the same time, our work in neurostimulation of slow-wave sleep is showing promise with a correlation between neurostimulation response, amyloid response, and memory in healthy older adults[1], as well as tolerance of stimulation in people living with Alzheimer's [2]. More studies to be done, but if you're curious, we link to a large body of research on our website https://www.affectablesleep.com/how-it-works?type=All#resear...
[1] https://doi.org/10.1093/ageing/afad228 [2] https://doi.org/10.1016/j.jagp.2024.07.002
This is not true.
Ozempic appears to affect the brain's rewards system and its known to decreased cravings and urges for a range of unhealthy behaviors, from alcohol consumption and smoking to gambling and shopping to nail biting and skin picking.
Beyond that, Ozempic appears to lower the risk of heart attacks and strokes in overweight people well beyond what weight loss alone would explain. Maybe due to the above (less drinking and smoking) or another unknown mechanism of action.
https://www.scientificamerican.com/article/weight-loss-drug-...
There is definitely massive variance in the individual psychology/biology that leads to habitual alcohol overuse so I'm sure others might not have the same experience. But for me I'm pretty confident that breaking that deeply engrained habit of starting the first of 6-10 drinks at 6-7pm every day was what did it (without feeling like I was being forced to do something I didn't want). Which was pretty much impossible for me to even envision back when it was such a normal part of my day-to-day coping strategy for stress/depression/etc.
Although I always knew my drinking was excessive and terrible for my health, past my early 20s I was super high functioning and wasn't interfering with my job or life (other than holding me back and probably slowly killing me), and so being an "alcoholic" was never part of my identity (rightly or wrongly), which I kinda think ironically made it easier to just take the win and move on with my life without nagging self-doubt or fixation on whether my "addiction is cured".
But it's been about 2 years now and I hardly ever think about alcohol even when super stressed so something, somewhere in my brain changed thanks to tirzepatide and whatever the mechanism I'm grateful for that happy accident of a positive side effect!
Do you plan on staying on a 'low dose' of semaglutide Ad vitam æternam ?
I'm asking because I believe that's one of the negative of these kind of drugs, it's effective at losing weight but as soon as you stop you gain back all the weight whereas learning to eat healthy is slower but more durable.
In my personal experience I've now known about 12 people who've taken it and stopped, and none have "rapidly" regained, in fact many have retained most of their loss for significant periods of time. Most people gain weight over a long period of time (from lets say early teen to their current age).
What happens when they stop is a very slow return to baseline gain. So if it took them 10 years to become obese, then it takes 6-12 months to lose it all with Tirzepatide, you'd expect it would take them 10 years again to regain it.
People act like this is some sort of addiction, but I don't think so - and I'd bet that a "refresher" that was only a small % of the year would keep most people completely at baseline, and they could even slowly taper that down.
I'd probably just go back to Keto if I decided or was forced to stop a GLP-1a completely. Keto was the first and only way I've had success losing weight in my life. But once the initial novelty wears off it takes a lot of discipline to stick to and continually avoid the pressure from friends/family to eat with everyone else. I'm also vaguely concerned about cholesterol impact long term doing it for life, but relative to obesity probably still a good trade off.
It's definitely doable though, I did it for 2 years so I know the drill and that's my fallback. But not being obese is much more enjoyable than being obese, and it's a lot easier to exercise at a normal weight, so I don't have much interest in going back to 260 pounds. If that meant taking a drug for life, so be it unless it turns out to cause turbo-cancer or something.
I mostly eat "healthy" foods by preference (and habit from growing up in a "health food" family), but for me my problem is managing portion control while never feeling completely full at the target calories per meal/day. Which can feel pretty miserable to stick with especially comparing to others in my family who more or less eat the same foods but don't have that problem at all. Keto was so effective because I actually felt "full" (at the expense of excluding a lot of otherwise healthy but carb-rich foods).
Taking Zepbound definitely reshaped my perception of obesity though, compared to Keto which required constant, intense self-enforced discipline avoiding 4/5 of any menu, being on a GLP1-a and able to eat what everyone else is eating but just stop and not feel hunger pains or cravings convinced me the attitude of "fat=lacking discipline" is antiquated and ignores real variance in how different people experience hunger/satiation.
Well I always assumed that people are fat because they are eating too much...of the wrong thing.
I lost 10kg not long ago, 20 lbs in American, and never ever i did feel hungry. Quite the opposite, i would be stuffed to the nose on fruits, vegetables and meats.
And believe me when I tell you I ate like an ogre.
I challenge anyone to actually gain weight on eating only vegetable fruits and meat. After losing these 10kg, I tried to gain 15kg of muscle and overeat on this regime to the point to want to vomit, couldn't gain weight. When I added fat and cereals, weight increased so fast I had to slow down.
With the average caloric expenditure being 2200 kcal for a normal healthy man, not even doing sport, the average vegetable being 300 kcal per kg, it means you would have to eat 7.3kg (16lbs) of vegetable per day.
I don't know you personally but I can safely say that you can't eat 16 lbs of vegetable per day, or 5lbs per meal. It's physically impossible.
So yeah I guess that how people experience hunger/starvation could play a role, but it's not the full story.
A couple years before starting Zepbound I had tried a prescription for naltrexone for 3 or 4 months to reduce drinking which had pretty much zero effect for me. Naltrexone apparently helps for some people and has a similar theorized mechanism acting on reward/pleasure but didn't do anything to break that habit of pouring a drink within the first hour I was back home.
I might have drank slightly less as it was slightly less enjoyable but did nothing for the habitual element which for me was much more problematic than how the alcohol made me "feel" subjectively or the exact number of drinks I had per night.
After I started Mounjaro, I haven't really had the urge to play at all. I played a game a few weeks ago but I was kind of "meh" about it, and haven't played since. It's striking.
A few friends and I made a maker community, and over the weekend I made a semi-automated newsletter for links we post in our Discord (https://themakery.cc). I really had fun doing that, it was great.
Last few weekends, https://encyclopedai.stavros.io/, https://theboard.stavros.io/, https://pine.town/, and a few other bits and pieces.
But yes, it's very probable (in fact we already know) the drug is doing several things in the body.
Nothing about justice was implied, so lets say desirable and undesirable instead of good and bad.
involves vascular inflammation. in the brain in the case of alzheimers. <theorized.> more readily applicable to vascular dementia.
and then, in the rest of the cardiovascular system in artherosclerosis/CVD. (reducing inflammation = reducing plaques laid down over them , that are being attracted to inflamed areas.. or piling up dead macrophages and foamy cells that went there to help.)
im not aware that either of these are totally settled at this time other than some anecdotal data on slowing down MACE and progression in the latter case (CVD). some cardiologists are believers and incorporating it in treatment now. its not an industry best practice but for those who are prescribing it for this reason, theyre citing a 20-40% reduction in events over 2-5 years.
or put another way. we know inflammation plays a role in CVD and we have a pretty reliable biomarker (CRP ) for whether this holds water and the inflammation is reduced by glp-1 agonists. not to be controversial or speak to medical matters but its my understanding that it does.
its role in dementia/alzheimers is just one of the ideas out there but the reasoning and the conclusions are kind of in the same neighborhood.
Alzheimer's isn't one thing but a category of degenerative pathologies.
Probably also requires holistic improvements in lifestyle ( hydration, sleep, exercise, diet (not just quantity)), gene in/activation, &| vaccines for TAU &| β-amyloid.
PS: I wonder if nootropics will be developed to emulate or enhance the effects of exercise.
{kind=link}