Wikipedia lists much lower numbers on https://en.wikipedia.org/wiki/Long_COVID (6–7% in adults, ~1% in children, less after vaccination.) and seems to use a more liberal definition than this paper, as it mentions "Most people with symptoms at 4 weeks recover by 12 weeks" (while the paper only considers it "long COIVD" if symptoms last past 3 months).
I've found studies (peer reviewed, as far as I can tell) claiming anything from well under 10% to well over 30%.
What's going on here?
Most people don't exploit the full capacity of their bodies and so would never notice, which is essentially the point OP is making. This disease very likely ravaged the 20% claimed, but the vast majority may never know because they're just never pushing their bodies hard enough.
If anyone wants to quantify this then Athlinks is a good place to start for race results. Obviously the data is somewhat noisy, like you'd have to throw out the slower finishers who maybe weren't trying hard. But if there's a significant correlation then it ought to show up.
Poor performers and no shows are exactly the population you’re looking for. To be clear the argument isn’t about a 10% decline across the board among people with long COVID as there’s non cardio pulmonary symptoms like brain fog, loss of smell, and difficulty sleeping.
If 80% of the fit population had COVID, 20% of them had long COVID, and half the people with long COVID had a 10% decline in race performance. That’s something like an overall 0.8% drop of performance assuming nobody dropped out or joined, but again you’re loosing people on both sides who were most impacted. Thus I’d be highly skeptical of finding an actual connection here rather than something else that impacts more people.
A more useful approach is to take a cohort of people who raced in 2019 and track what happened to every single one of them specifically.
The PVCs, adrenaline dumps, sleeping problems and anxiety/panic were insane! The doctor thought that my hypothalamus was inflamed because of COVID.
When you mention “adrenaline” was this somehow tested or just a frequent feeling of being stressed when you had no reason for such?
I find finding the right type of specialist isn’t always straightforward and even when one does, about 80% of the time they aren’t interested in diagnosing anything not blatantly obvious…
If long COVID disproportionately affects people who are sedentary, then you won't see that in endurance athlete performance.
After 5 years I would happily trade only a 10% performance loss for the days and nights full of nerve damage pain (neuropathy)and what seems to be 30% performance loss
BTW very relevant to your daughter's story:
the first year of long-covid I was absolutely certain I had permanent lung damage and started searching everywhere for solutions
There are two possibilities that might be hopeful for her
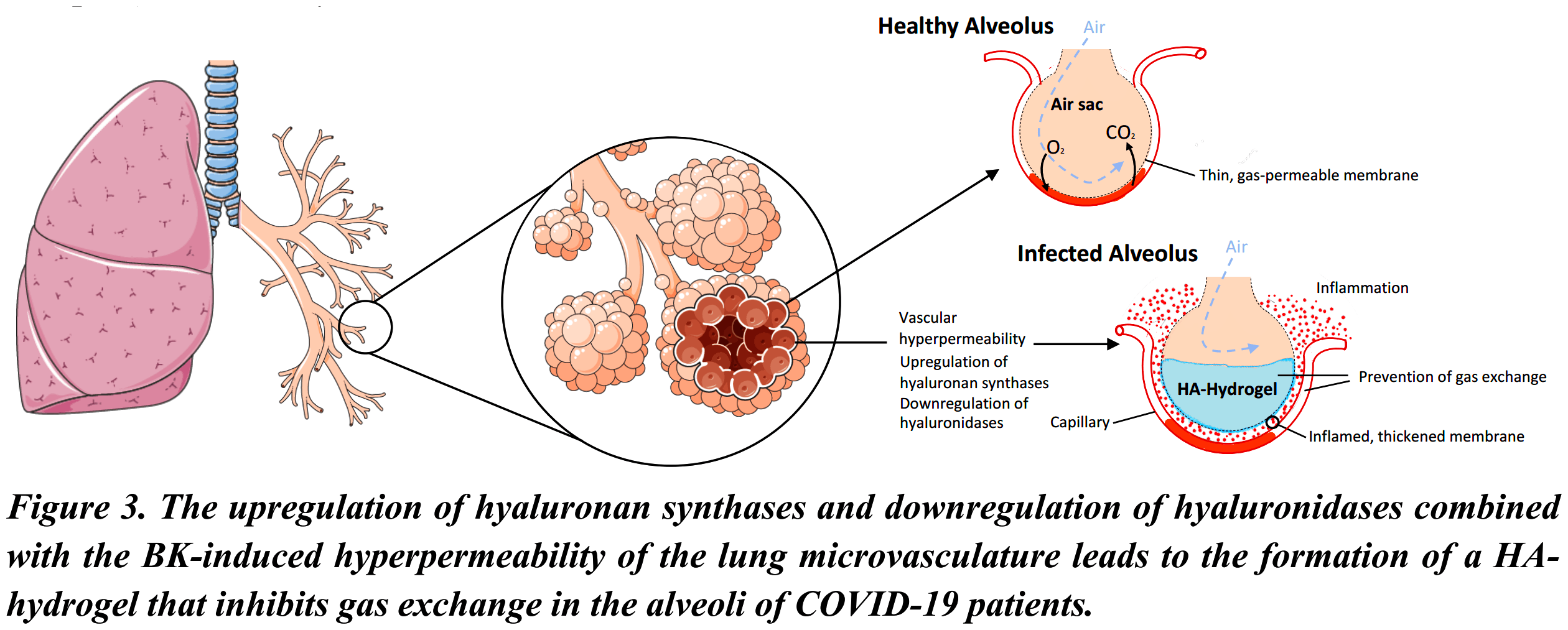
The first is that it might not be permanent alveoli damage (which do not regenerate in humans) but rather obstruction from a "hydrogel" that forms during active covid and takes many many months if not years to dissipate entirely
1. https://images2.imgbox.com/98/e1/gw8bO0ug_o.png
The second is much more serious and not available in the United States except experimental trials for other diseases
2. "Inhaled Tissue Plasminogen Activator" or "Nebulised Rt-PA"
https://www.google.com/search?q=Nebulised+Recombinant+Tissue...
https://academic.oup.com/qjmed/article/113/8/539/5818885 (look at the photos in this second link)
BUT there's something you can try right away
see this table of plasminogen activators
* https://pmc.ncbi.nlm.nih.gov/articles/PMC5553328/table/t0001...
at the bottoms is Nattokinase and Serrapeptase
which are simple enzymes, you can buy Natto-Serra on Amazon and very very slowly perhaps over many months it might help her lungs (this is just a guess)
> The first is that it might not be permanent alveoli damage (which do not regenerate in humans) but rather obstruction from a "hydrogel" that forms during active covid and takes many many months if not years to dissipate entirely
I didn't go into too much detail in my original post, but we think this is likely what happened to my daughter. Post-COVID, she could still go for long durations at 80% but when she pushed her limits, she would hit a wall and start to experience asthma like symptoms along with the feeling like she had mucous in her lungs that she couldn't get out. It took close to 2 years for her to stop experiencing those symptoms, at which point her competitive running peers had passed her by. She's happy to be able to enjoy running again but she did lose out on the competition part.
Additionally, a lot of those numbers are based on earlier strains of COVID, which were much more severe.
I suspect the 1/5 figure is largely true for "has some degree of cardiovascular damage and worsened general health after COVID", but the number of people actually disabled by the condition is much lower.
That said, any loss of ability is a sad thing, and I am incredibly disappointed that we did not introduce any shared indoor space air quality legislation post-pandemic.
Further, the studies on long COVID incidence in vaccinated vs unvaccinated people suggested that the rates in vaccinated individuals were lower, though iirc it was only by something like a third or half. (among people who were symptomatic, at least, the total protective effect was likely greater)
Majority of the studies on myocarditis after vaccination found very low rates, with close to zero moderate to serious cases, and a full return to baseline of whatever the metrics studied were, I don't remember.
Long COVID associated with SARS-CoV-2 reinfection among children and adolescents in the omicron era
https://www.thelancet.com/journals/laninf/article/PIIS1473-3...
(The same omicron era the media originally claimed was "not as bad as previous variants." Perhaps not in the acute phase, but as we've seen, that's the least of anybody's concerns who track the longterm risks.)
> I am incredibly disappointed that we did not introduce any shared indoor space air quality legislation post-pandemic.
That seems like a tempting thing to lament, and I did too until seeing this recently:
Study finds HEPA purifiers alone may not be enough to reduce viral exposure in schools
https://www.eurekalert.org/news-releases/1101354
This suggests our most reliable protection to date is consistent N95 usage (since present vaccines don't reliably prevent transmission) until next gen vaccines are developed.
Agreed. In fact, even before COVID this was long overdue to be addressed in classrooms etc:
> ventilation to reduce rebreathing and CO2 levels
Unfortunately since that hasn't happened yet, methods like:
> In-line far UV sterilisation
> HEPA
are not effective. It isn't that they don't kill/stop the virus. The problem traces back to the inadequate forced air exchange and distribution which these methods require, and which is often a show stopper when you're talking about retrofitting existing structures without costs becoming insane. At a certain point it's easier to build new with these things in mind (and we absolutely should be taking requirements to do so more seriously).
> might not be enough as a single-building intervention, but it would almost definitely change disease spread dynamics if deployed world/nation wide.
The point of the previously linked study is to demonstrate that "something is better than nothing" reasoning doesn't always apply. We need to go big to see an actual measurable improvement over longer time spans. Otherwise, what's the benefit seen if you delay an average (but inevitable) infection from occurring by X days? There basically is none.
It reduces the R0 factor, which reduces the amount of people that need to be resistant for herd immunity to take place, and which makes it easier for other measures to bring it down further, potentially below 1 where the disease dies out instead of continuing to spread.
The results of the study suggest it doesn't, as measured by outcomes:
> While we did not find an association between HEPA purifier use and high overall viral exposure, the intervention was associated with a 32.8% reduction in viral diversity. However, the clinical significance of these changes is not clear given that we did not find an association between viral diversity and school absenteeism.
Point being, it only takes a very small dose of a aerosol borne virus to keep it in circulation. Breaking this chain requires extreme measures. Not impossible to achieve, but not trivial, either. Considering the widespread damage that long COVID is causing, I sincerely hope we find a way.
There are probably a lot of syndromes caused by latent infections from virii like EBV, various herpes, HPV, etc that don't go properly diagnosed or treated if they can be treated at all.
Also, it's been found that some viral infections retreat to tissues where their detection might be difficult/impossible without biopsy. You saw this with, for example, Ebola, where survivors could test negative for the virus, but it would still survive and replicate in different isolated tissues like those in the eye.
Never enough to warrant going to a doctor unless I was being super paranoid (and spend a long time convincing them I wasn't paranoid) but just enough to always wonder if there was something more to the story.
I started having heart flutters a day or two after my shot and had severe fever (I was 25 at the time), but the former never went a way. I brushed it off as a temporary symptom and typical after shot reaction (well, fever was at least). Heart flutters never went away and I didn't go to the doctor for at least a few months, it became so frequent that I could not sleep, exercise or even climb the stairs anymore without heart feeling like it's about to explode out of my chest. Not the high heart rate, but abrupt, irregular vibrations/twitching and sometimes feeling like you get punched in the chest, just from the inside around the heart area. Anyway, it happens frequently and in any situation, even at rest.
Got diagnosed with third degree AV block. The flutters were due to the significant damage to the heart muscle, which caused the failure of the conduction system - signals from the upper chambers did not always reach the lower chambers.
I am not angry at anyone or anything, just disappointed. It would feel a lot easier if it was some obvious bad decision of mine, like drinking, doing drugs, smoking, or being overweight, but I did not nor were any of these things. I still keep categorizing life as "before" and "after".
For instance, a disproportionate amount of long COVID cases are reported by women between the ages of 40 and 60, the exact age range when most women experience menopause [0]. Menopause can cause brain fog, fatigue, and other symptoms that mirror those of long COVID. Since pretty much everyone has had COVID, it’s a basic statistical certainty that many women caught COVID exactly when their menopausal symptoms started (whose onset can be extremely sudden), and falsely causally associate the two. The exact same conflation likely happens in children, who also go through several profound developmental shifts.
[0] https://telegraph.co.uk/news/2022/12/28/long-covid-may-actua...
It is possible, but not to the degree that all long Covid cases are being confused with external factors.
> Menopause can cause brain fog
Additionally, long Covid can cause brain fog. This was shown in brain scans from a popular HN post about a research paper just yesterday:
https://news.ycombinator.com/item?id=45539845
Those patients were 20-59 and had "no previous history of neuropsychiatric disorders."
Didn't mean to imply that all cases are, just that our definition of and knowledge about long COVID is nebulous enough that some nontrivial proportion of cases are likely attributable to external factors.
>Additionally, long Covid can cause brain fog. This was shown in brain scans from a popular HN post about a research paper just yesterday
Absolutely, just as other infections can cause severe lingering symptoms [0]. But we don't really know how prevalent these are, nor the severity of the prevalence. Studies like the one you link typically select for the most severe cases. We don't know whether it's useful to generalize from those.
[0] https://en.wikipedia.org/wiki/Post-acute_infection_syndrome
39 year old male. I was in great shape both physically and mentally before my trip.
https://www.newsonhealth.co.uk/
over research from Harvard.
One, maybe two non-research docs or... a team of research docs.
[0] https://jamanetwork.com/journals/jamanetworkopen/fullarticle...
Perhaps its a reflection of how hard it is to get the medical community to take Long COVID seriously ?
I would say there is more chance of them (sadly) telling you to go home, take a couple of paracetamol and get some rest. Or if you're lucky, they might mis-diagnose you with something else....
(No first-hand experience here, just going by one or two anecdotal stories I've heard on the grapevine)
Well let’s think about why. You’ve got an illness (Long COVID) that you can’t detect and manifests itself in a myriad of ways, most of which are very vague and subjective (“brain fog” or “I can’t exercise as much as I used to”) and also not detectable.
Is it any wonder doctors might think of it as today’s fibromyalgia?
The same will happen for Long Covid and ME/CFS, the diagnostics are there in research, they even show up in scans and tests that can be run in healthcare systems today, its just there is a resistance to run them.
There are a myriad of illnesses here that this seems to apply to.
For a variety of reasons, hyping the threat of infection has been a pretty widespread practice among the medical and scientific community since COVID began. There's no way on earth 1 out of 5 kids are still experiencing symptoms 3 months out.
I don't see how you'd know the exact number without a solid diagnostic check.
> Long COVID (LC) impacts one in five children after an acute SARS-CoV-2 infection
So, 20% of children that suffered of an acute SARS-CoV-2 infection, did not recovered immediately, but experienced also Long COVID.
Maybe not all infections are considered "acute".
Maybe you are not the type of person that people feel comfortable to share their health problems information with.
Anyway, having had long covid myself for over 15 months, there are many, many people suffering with it, we are just discovering the tip of the iceberg
Anyway, because of the stratification many people don’t know anyone with long covid, while at the same time half of my friends have it. Both can be true observations of our surroundings.
On the actual numbers I would say that ~10% get some level of Long Covid while half of those recover in the first year. Of those who don’t recover around half have GJH which is a massive over representation suggesting a strong predisposition.
[1]https://www.sciencedaily.com/releases/2012/05/120529211645.h...
"the patients who gave blood had a significant reduction in systolic blood pressure (from 148 mmHg to 130 mmHg) as well as reduction in blood glucose levels and heart rate, and an improvement in cholesterol levels (LDL/HDL ratio)."
https://pmc.ncbi.nlm.nih.gov/articles/PMC8994130/
The study specifically does not look at the effect on recipients, though the donation centers do not disallow such donations. My presumption is that the donation is a net positive all around. If study comes to show the contrary, I'll certainly revise my approach.
And from what I understand, PFA contamination has no bearing on whether or not you can donate.
I didn’t live in an urban area until I was in my late 20s.
The latter was given a scientific explanation in modern times: the webbing contains live penicillium fungi in quantities sufficient to act against microbes.
https://my.clevelandclinic.org/health/treatments/24197-plasm...
There are also claims that it improves dementia / Alzheimer's symptoms and popular "longevity biomarkers".
I think you just need to reach for a literature that's a few hundred years older maybe.
If so, the answer is that the body replenishes plasma in a day and red cells in six weeks (redcrossblood.org FAQ). The relative amount does change quickly.
Even if they did, the hormonal effects would likely swamp anything else. Which is a huge problem: women are routinely excluded from studies to avoid that, meaning we have no idea what the effects are on women.
OP's linked paper has "the iron-reduction patients had 300ml of blood removed at the start of the trial and between 250 and 500ml removed four weeks later."
A blood donation removes 500 ml, so about a year of menstruation all at once. You can donate every two months, besides.
So, yes, if there is an effect then we might expect the magnitude of the effect to differ. Or else we'd expect a paper cut to also have the same effect.
Sex biological difference could matter as well.
If this works, how is anyone going to make money off of it?
---
The title should be edited. It sounds as if the test is 94% accurate at detecting long covid, but in fact it's 94% accurate at counting microclots
> We estimated a 94% accuracy for the microclot count using the devices, significantly higher than the traditional counting of microclots on slides (66% accuracy)
> We evaluated the diagnostic power (...). We estimated a 94% accuracy for (our method), significantly higher than the (traditional method) (66% accuracy).
Both methods have counting in their name, but they are comparing the diagnostic power.
https://www.ssph-journal.org/journals/public-health-reviews/...
> Prevalence estimated (...) 2%–3.5% in primarily non-hospitalized children.
So a fake test always saying "No" would be more accurate at 96.5% accuracy.
The sample size is pretty small here and the control group even smaller. The paper concludes that a larger study is necessary to confirm the result.
The title on hn which implies that seems to be inaccurate and it's not the original title of the article.
> We evaluated the diagnostic power of the device in a cohort of 45 LC patients and 14 healthy pediatric donors. We estimated a 94% accuracy for the microclot count using the devices, significantly higher than the traditional counting of microclots on slides (66% accuracy).
They are comparing the predictive power and using accuracy (instead of sensitivity, recall, F1, etc.). For their method "using the devices", they compute an accuracy of the predictive power, not of the count, of 94%. For the previous method they say the accuracy is 66%.
Basic questions: Is accuracy even a good metric for this? Is 94% a good value or just the difference between bad and very bad?
It might very well be that their improvement is from bad to really good, but the point is that a raw stat of "94% accuracy" is useless without context and so is the headline.
See https://www.sciencedirect.com/science/article/pii/S155608641...
> In general, an AUC of 0.5 suggests no discrimination (i.e., ability to diagnose patients with and without the disease or condition based on the test), 0.7 to 0.8 is considered acceptable, 0.8 to 0.9 is considered excellent, and more than 0.9 is considered outstanding
So .94 is actually extremely good.
Tests have a sensitivity (1 - percentage of false negatives) and specificity (1 - percentage of false positives)
"Accuracy" usually refers to sensitivity. If specificity is near 100% and the test is cheap/fast even low sensitivity can be good
On the other hand you could have sensitivity of 100% but the test could be useless if specificity is low and the condition is rare
https://pmc.ncbi.nlm.nih.gov/articles/PMC4614595/#:~:text=Ac...
That is exactly why I gave the trivial example of an "always No" test. It has perfect specificity (zero false positives) and has accuracy corresponding to prevalence. The sensitivity is zero, however, which is the point.
Junk science?
The primary conclusion of this research was basically just "this looks like it would be worth doing more research on." Which is a fair conclusion for a study this small.
Obviously there's some probability this is all coincidence but it does seem strange, especially considering the predisposition for these people to not think their issues were triggered by covid infection.
Its not a big unknown anymore, its very prevalent, it has a lot of symptoms, it has a clinical definition but its problematic and there are many diagnostic tests that can detect parts of the condition but none has yet reached sufficient prominence to be adopted by healthcare. Healthcare is largely ignoring that Long Covid exists so you can't get diagnosed with it but its very much a real thing and a lot of people have it.
[1]https://www.who.int/news-room/fact-sheets/detail/post-covid-...
> Approximately 6 in every 100 people who have COVID-19 develop post COVID-19 condition
vs., for example:
> From one center in Wuhan, 1,359 survivors completed 3-year follow up and 54% had at least one persistent symptom of Long Covid
This only underscores the lack of clinical definition. Both of these suffer from the same fundamental error, which, again, is that there's no precise definition of the syndrome. They include symptoms that are common amongst healthy people, mix them with less-common things that are associated with Covid (e.g. anosmia) and try to call this a disease state. See the WHO's grab-bag list of possible inclusion criteria:
> Over 200 different symptoms have been reported by people with post COVID-19 condition. Common symptoms include: fatigue, aches and pains in muscles or joints, feeling breathless, headaches, difficulty in thinking or concentrating, alterations in taste.
So literally having "headaches" or "aches and pains" is enough to claim Long Covid, according to the WHO.
The Topol/Aly substack engages in the same logic, and you will see that the referenced charts and graphs cover everything from fatigue to heart attack. Aly, in particular, has based his entire long covid research on a single dataset of (largely elderly, unhealthy prior to infection) VA patients that he refuses to release, and routinely engages in statistical fishing expeditions for new "symptoms" within that dataset.
https://yourlocalepidemiologist.substack.com/p/long-covid-re...
Excellent, a new way to test for the "fibrinaloid clots", a term that has only recently appeared in the literature since 2022, directly after the first experimental injections were administered worldwide and 2 years after the declared pandemic. It sounds like the authors are assuming "long Covid" comes from Covid rather than the experimental injections without ever having ruled out the latter, even though the onset correlates temporally with the experimental injections far more than the declared pandemic. Since this term never existed in the literature during the first 2 years of the declared pandemic, and only finally appeared in 2022 (and only in 1 article) before it started gaining traction, we must ask ourselves the following questions if we are truly interested in pursuing the scientific method: 1. Did the authors categorize the test subjects by those who had received the COVID-19 injection and those who had not? 2. If not, how do we rule out these effects being long-term effects from the experimental injections which cause people's bodies to continually produce the Spike protein the authors discuss in their paper as being the cause of the "fibrinaloid clots"? 3.Isn't this continual production of Spike induced by the injections something that should be controlled for to answer the question one way or another?
Suggestions: Test for "fibrinaloid clots" in subjects who have had confirmed COVID-19 and categorize them by how many experimental injections they received; include patients who received none. Then plot the number of experimental injections per patient on the x axis and the detected microclot size on the y axis.
Best regards to all.
Likely because you're attempting to spread some form of anti-vax nonsense.
They are looking into that.
At least, that's my layman's understanding when I was following it some years ago. I'm not sure if there's been more recent studies that have found more concrete links since then, but I suspect GP is in the same boat, which is why they asked.
{kind=link}